ACL RUPTURE
ANATOMY AND MECHANISM
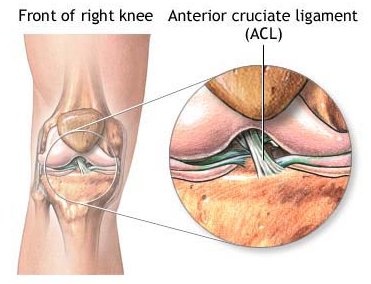
The anterior cruciate ligament (ACL) of the knee attaches to the back of the femur (thigh bone) and front of the tibia (shin bone) and is one of the main stabilisers of the knee. It prevents excessive movement of the tibia forward in relation to the femur, and also provides some rotational stability.
It is commonly injured in sports such as netball and rugby, when stopping suddenly. For example being tackled in rugby, when the lower leg is suddenly immobilised and the knee hyper-extends.
The ACL may be strained (only some of the fibers torn) or ruptured (all of the fibers torn).
SIGNS AND SYMPTOMS
- Pain
- Instability (feeling that the knee may “give way”)
- Immediate severe swelling
- Audible “pop” sound at time of injury (with a ruptured ACL)
- Difficulty walking
- Limited range of movement
TREATMENT
Immediate treatment, and within the first 3 days, consists of the RICE principles:
Rest – rest the knee, avoid too much walking and refrain from playing sport.
Ice – Every 2 hours apply ice, this will help with the pain and swelling.
If using an ice pack (or frozen peas), leave it on for 10-20 minutes, using a tea towel or similar between the pack and skin to prevent ice burn.
If using an ice cube, “massage” your knee with the ice, gently rubbing it over the skin. Keep the ice cube moving to prevent ice burn and do this for no longer than 5 minutes.
Compression – Use Tubigrip if you have some on the knee to apply some compression, this will help to alleviate the swelling.
Elevation – Prop your leg up so that your knee is elevated above the level of your heart. This will help to minimise the swelling.
If the ACL is strained treatment will likely be conservative (non-surgical). If the ACL is ruptured treatment may include surgical repair of the ligament or conservative treatment.
Surgery is often recommended to athletes who intend to continue competing in demanding sport. This involves a reconstruction of the ligament rather than a repair, where a graft is taken from a hamstrings tendon or the patellar tendon and replaces the ruptured tendon. This is done arthroscopically (key-hole surgery).
Following surgery it will be at least 6-9 months before you can return to sport and you will require physiotherapy rehabilitation. This will initially include exercises to return the joint’s normal range of motion, followed by a strengthening programme which is gradually progressed to introduce more stressful/demanding activities and, finally, a functional programme aimed at sport-specific activities to aim for returning to playing sport.
If you do not have surgery, physiotherapy rehabilitation will still be important. This will consist of exercises to retain the joint’s range of motion, reduce swelling and increase strength of the muscles around the knee in order to increase stability. You may still be able to play some sport, but this will need to be discussed with your physiotherapist and/or specialist.
Leave a reply

{kind=link}
{kind=link}
Leave a reply